Support our educational content for free when you purchase through links on our site. Learn more
🫀 Bioprinting Human Organs: The 2026 Roadmap to Saving Lives
Imagine a world where the agonizing wait for a donor heart is a thing of the past, replaced by a printer in your local hospital humming away, crafting a perfect, living organ from your own cells. It sounds like the plot of a sci-fi novel, but at 3D Printed™, we’ve seen the blueprints, and the future is already being printed layer by layer. While we can currently fabricate simple tissues and hollow structures like bladders, the quest to print complex, solid organs like hearts and livers remains the “Mount Everest” of bioengineering.
In this deep dive, we peel back the layers of bioprinting human organs, exploring the revolutionary bioinks, the vascularization bottleneck that has stumped scientists for decades, and the ethical quagmires we must navigate. We’ll reveal why hollow organs are the “low-hanging fruit” while solid ones remain elusive, and we’ll share the latest breakthroughs from labs like Harvard and Rice University that are finally cracking the code. By the end, you’ll understand exactly how close we are to the day when organ rejection becomes a relic of history.
Key Takeaways
- The Vascularization Wall: The primary hurdle preventing the printing of solid organs is creating a functional network of blood vessels to keep internal cells alive; without it, the organ dies within minutes.
- Hollow vs. Solid: We are already successfully printing and implanting hollow organs (like bladders and tracheas), but solid organs (hearts, kidneys) remain in the experimental phase due to their complexity.
- Personalized Medicine: Using a patient’s own stem cells eliminates the risk of immune rejection, potentially ending the need for lifelong immunosupressant drugs.
- Current Reality: While full organ transplants are likely 10–20 years away, organ-on-a-chip models are already revolutionizing drug testing and saving animal lives.
- Ethical & Economic Shifts: As the technology matures, society must address critical issues regarding equitable access, cost, and the moral implications of manufacturing human life.
Table of Contents
- ⚡️ Quick Tips and Facts
- 🧬 From Sci-Fi to Reality: A Brief History of Bioprinting Human Organs
- 🏗️ The Blueprint: How 3D Bioprinting Technology Actually Works
- 🧪 The Ink Matters: Exploring Bioinks and Living Cell Sources
- 🖨️ Top 7 Bioprinting Techniques Revolutionizing Organ Fabrication
- 🫀 The Hollow Challenge: Progress in Bioprinting Human Hollow Organs
- 🧠 The Solid Hurdle: Vascularization Strategies for Complex Solid Organs
- 🔬 Current Breakthroughs: What We Can Print Today vs. Tomorrow
- ⚖️ Ethical Quagmires: The Moral Implications of Printing Human Organs
- 💰 The Cost of Life: Economic Bariers and Future Accessibility
- 🛡️ Regulatory Roadblocks: FDA Approval and Safety Standards
- 🌍 Global Landscape: Leading Labs and Companies in the Race
- ❓ Frequently Asked Questions About Bioprinting Human Organs
- 🏁 Conclusion
- 🔗 Recommended Links
- 📚 Reference Links
⚡️ Quick Tips and Facts
Before we dive into the deep end of the cellular pool, let’s splash around with some hard-hitting facts that might just blow your mind (or at least your current understanding of biology).
- The Waiting List is Real: Over 103,0 people are currently on the US waiting list for organ transplants. Every 9 minutes, someone is added, and tragically, 17 to 20 people die every day waiting for a match. Source: UNOS
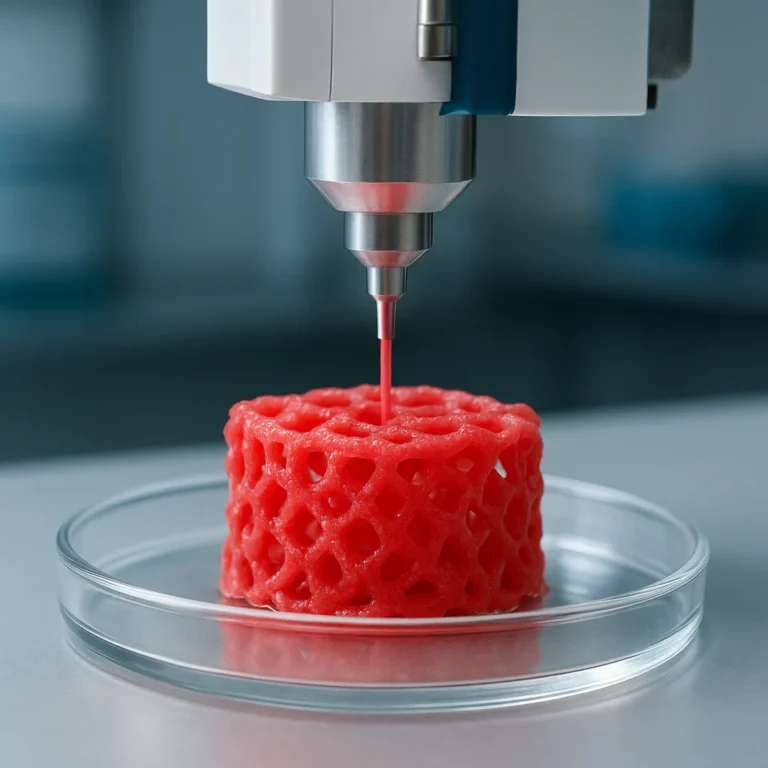
- It’s Not Just “Printing”: Bioprinting isn’t like your FDM printer spitting out a plastic figurine. It involves living cells, bioinks, and scaffolds that must survive the printing process and then grow into functional tissue.
- The “Hollow” vs. “Solid” Divide: We are surprisingly good at printing hollow organs (like bladders and tracheas) but hitting a massive wall with solid, vascularized organs (like hearts and livers) because of the need for complex blood vessel networks.
- Cost Reality Check: While a standard 3D printer might cost a few hundred bucks, a research-grade bioprinter can set you back anywhere from $130,0 to $30,0+, and the “ink” (bioink) can cost upwards of $10 per gram.
- The “Heart on a Chip” is Here: We aren’t just dreaming; scientists at Harvard have already created a 3D-printed heart on a chip that beats spontaneously. It’s not ready for your chest, but it’s ready for drug testing. Source: Wyss Institute
Wait a second… If we can print a beating heart on a chip, why can’t we just print a whole heart for a patient tomorrow? The answer lies in a tiny, invisible problem called vascularization, and we’re going to unpack exactly why that’s the “Holy Grail” of bioprinting later in this article.
🧬 From Sci-Fi to Reality: A Brief History of Bioprinting Human Organs

Remember the days when 3D printing was just a novelty for making plastic trinkets and failed phone cases? We were there too! But the journey from printing a PLA dragon to printing a living human organ is a story of rapid, almost dizzying evolution.
The Early Days: Stereolithography and the First Spark
It all started in 1986 with Chuck Hull’s invention of stereolithography (SLA). While Hull was focused on curing photopolymers with UV light, the medical community was quietly dreaming of something bigger. The concept of layer-by-layer biological fabrication was born, but it took decades to move from theory to practice.
The 20s: The First “Printed” Tissues
Fast forward to the early 20s, and the first 3D bioprinted tissues emerged. In 202, researchers at Wake Forest University successfully printed a human bladder using a patient’s own cells. It was a watershed moment! This proved that we could use a patient’s cells to create a functional organ, effectively bypassing the risk of immune rejection.
The 2010s: The Bioink Revolution
The real game-changer came with the development of sophisticated bioinks. Early attempts used simple hydrogels, but they lacked the structural integrity to hold complex shapes. Enter FRESH (Freeform Reversible Embeding of Suspended Hydrogels), developed by Professor Adam Feinberg’s team. This technique allowed scientists to print soft, delicate structures (like heart valves) by supporting them in a gel bath that could be melted away later.
Fun Fact: The first YouTube video that really captured the public’s imagination about this tech (which we’ll link to later) showcased the SLATE technology from Rice University, demonstrating how they could print entangled cardiovascular networks that mimic the body’s natural passageways. It was the moment the “impossible” started looking “inevitable.”
Today: The Race for Complexity
Now, we are in the era of multi-material printing and organ-on-a-chip technologies. We can print skin grafts, cartilage, and even complex liver tissues for drug testing. But the ultimate goal—printing a fully functional, transplantable human heart or kidney—remains the “Mount Everest” of the field.
🏗️ The Blueprint: How 3D Bioprinting Technology Actually Works
So, how does this magic happen? If you’ve ever struggled with bed leveling on your Ender 3, you know that precision is everything. Bioprinting takes precision to a whole new level because one wrong move means dead cells.
Step 1: The Digital Twin (CAD & Imaging)
It starts with the patient. Using CT scans or MRI data, engineers create a 3D digital model of the missing organ. This isn’t just a shape; it’s a map of where every cell type needs to go.
- Software Tools: We use advanced CAD software like Materialise Mimics or 3D Slicer to segment the medical images.
- The Challenge: Unlike a plastic part, an organ has heterogeneous cell distribution. The heart muscle cells need to be in the walls, while the blood vessel cells need to be in the channels.
Step 2: The Bioink Formulation
This is the “ink” that makes it all possible. A bioink is a mixture of:
- Living Cells: Often stem cells (like iPSCs or MSCs) or specific differentiated cells (hepatocytes for liver, cardiomyocytes for heart).
- Biomaterials (Hydrogels): These act as the scaffold, providing structure and nutrients. Common materials include alginate, collagen, gelatin, and fibrin.
- Growth Factors: Chemical signals that tell the cells what to do (e.g., “grow into a blood vessel!”).
Step 3: The Printing Process
The bioprinter deposits the bioink layer by layer. Depending on the technique (which we’ll cover in depth later), this can be done via extrusion, inkjet, or laser-assisted methods.
- Crucial Detail: The printer must maintain a sterile environment and precise temperature control (usually 37°C) to keep the cells alive.
Step 4: Maturation and Vascularization
Once printed, the organ isn’t ready for transplant. It’s a “baby” organ. It needs to be placed in a bioreactor—a machine that mimics the human body’s conditions (pulsing blood flow, nutrient supply, mechanical stress) to help the cells mature and form functional tissue.
The Big Question: We can print the shape, but how do we get blood to the middle of the organ? If the cells in the center don’t get oxygen, they die. This is the vascularization bottleneck, and it’s the reason we can’t print a whole heart yet. We’ll solve this mystery in the “Solid Hurdle” section!
🧪 The Ink Matters: Exploring Bioinks and Living Cell Sources
If your 3D printer is the car, the bioink is the fuel. And let me tell you, you can’t just put regular water in a Ferrari. The quality of your bioink determines the success of the entire operation.
Types of Bioinks: Natural vs. Synthetic
| Bioink Type | Examples | Pros | Cons |
|---|---|---|---|
| Natural Polymers | Collagen, Alginate, Gelatin, Fibrin, Hyaluronic Acid | High biocompatibility, supports cell adhesion, mimics natural ECM (Extracellular Matrix). | Weak mechanical strength, batch-to-batch variability, rapid degradation. |
| Synthetic Polymers | PEG (Polyethylene Glycol), PLA, PCL, Pluronic | Tunable mechanical properties, consistent quality, slow degradation. | Poor cell adhesion (often needs modification), potential toxicity of byproducts. |
| Hybrid Bioinks | Collagen + PEG, Alginate + Gelatin | Combines the best of both worlds: strength + biocompatibility. | Complex formulation, harder to optimize printing parameters. |
The Cell Source Dilemma: Where do the cells come from?
The cells are the “living” part of the equation. We have three main sources:
-
Autologous Cells (Patient’s Own):
Source: Skin or blood samples from the patient.
Pros: Zero immune rejection. The body accepts the organ as its own.
Cons: Time-consuming to culture, limited supply, potential for genetic defects. -
Alogeneic Cells (Donor):
Source: Donors (like blood transfusions).
Pros: Ready-to-use, scalable.
Cons: Risk of immune rejection, requires immunosupressant drugs. -
Stem Cells (The Magic Bullet):
iPSCs (Induced Pluripotent Stem Cells): Reprogramed adult cells (like skin cells) back to an embryonic-like state. They can turn into any cell type. No embryo destruction, huge ethical advantage.
hESCs (Human Embryonic Stem Cells): Derived from embryos. Highly potent but ethically controversial.
MSCs (Mesenchymal Stem Cells): Found in bone marrow and fat. Good for bone and cartilage, but harder to turn into complex organ cells.
Enginer’s Note: We’ve tried printing with spider silk proteins for cardiac tissue because of their incredible strength and biocompatibility. It sounds wild, but it works! However, sourcing enough spider silk for a human heart is… well, let’s just say we aren’t farming spiders in our garage.
🖨️ Top 7 Bioprinting Techniques Revolutionizing Organ Fabrication
Just like in the FDM vs. SLA debate, there is no “one size fits all” in bioprinting. Different organs require different printing techniques. Here are the top 7 methods currently shaking up the industry:
1. Extrusion Bioprinting
- How it works: A syringe pushes bioink through a nozzle using pneumatic or mechanical pressure.
- Best for: High cell density, viscous bioinks, creating large structures.
- Pros: Can print complex shapes, relatively low cost.
- Cons: Lower resolution, potential for shear stress that can damage cells.
- Viability: ~40-85% (depends on pressure).
2. Inkjet Bioprinting
- How it works: Similar to a standard office printer, but drops tiny droplets of bioink.
- Best for: High speed, low viscosity bioinks, patterning cells.
- Pros: Fast, high resolution, low cost.
- Cons: Limited to low-viscosity inks, clogging issues, lower cell density.
- Viability: >85%.
3. Laser-Assisted Bioprinting (LAB)
- How it works: A laser pulse hits a “ribbon” coated with bioink, propelling a droplet onto the substrate.
- Best for: High precision, nozzle clogging, high viscosity inks.
- Pros: Extremely high resolution (10 µm), no shear stress on cells.
- Cons: Expensive, slow, complex setup.
- Viability: >95%.
4. Stereolithography (SLA) / Digital Light Processing (DLP)
- How it works: UV light cures a photosensitive resin layer by layer.
- Best for: High-resolution scaffolds, complex geometries.
- Pros: Fast, high accuracy.
- Cons: UV light can be toxic to cells, limited to photopolymerizable bioinks.
- Viability: >90% (with modified inks).
5. Microfluidic Bioprinting
- How it works: Uses micro-channels to mix and deposit cells with extreme precision.
- Best for: Creating micro-tissues, organ-on-a-chip devices.
- Pros: Precise control over cell placement, low waste.
- Cons: Limited to small-scale structures.
6. SWIFT (Sacrificial Writing into Functional Tissue)
- How it works: Developed by Harvard, this prints a sacrificial ink into a dense matrix of living cells, then melts the sacrificial ink to leave behind vascular channels.
- Best for: Vascularization of thick tissues.
- Pros: Creates dense, functional tissues with blood vessel networks.
- Cons: Complex process, requires specific bioinks.
7. Co-axial Bioprinting
- How it works: Uses a special nozzle with two concentric channels to print a core-shell structure (e.g., a cell core surrounded by a structural shell).
- Best for: Creating hollow tubes (blood vessels, airways).
- Pros: Mimics natural vessel structure perfectly.
- Cons: Limited to tubular structures.
Pro Tip: If you are looking to experiment with bioprinting concepts at home (for educational purposes, of course!), check out open-source projects on Thingiverse or GitHub that adapt standard FDM printers for low-viscosity hydrogel printing. While you won’t be printing a heart, you can print scaffolds to understand the geometry!
🫀 The Hollow Challenge: Progress in Bioprinting Human Hollow Organs
Let’s address the elephant in the room: Why are hollow organs easier?
Hollow organs like the bladder, trachea, and urethra have a simpler structure. They don’t need a complex, branching network of blood vessels to keep every single cell alive because their inner surface is in direct contact with fluids (urine, air, etc.).
Success Stories in Hollow Organs
- The Bladder: In the early 20s, Dr. Anthony Atala’s team at Wake Forest University successfully implanted 3D-printed bladders into patients. They took a scaffold, seeded it with the patient’s own bladder cells, and grew it in a bioreactor. The results were promising, with patients showing normal function.
- The Trachea: Several attempts have been made to print tracheal scaffolds using PCL (Polycaprolactone) and PLA. While some early trials faced complications (like scaffold collapse or infection), the technology has evolved. Newer methods use dual-head printing to combine structural polymers with cell-laden hydrogels.
- Blood Vessels: Using co-axial printing, researchers can create micro-vessels that mimic the natural structure of arteries and veins. These are crucial for connecting larger organs to the body’s circulatory system.
The Remaining Hurdles
Even with hollow organs, challenges persist:
- Mechanical Strength: The printed organ must withstand the pressure of fluid flow without collapsing.
- Integration: The printed organ must integrate seamlessly with the patient’s existing tissue.
- Long-term Stability: Will the scaffold degrade at the right rate? Will the cells stay functional for years?
Did you know? The FRESH technique was originally developed to print heart valves, which are technically hollow structures. This success paved the way for more complex hollow organ research.
🧠 The Solid Hurdle: Vascularization Strategies for Complex Solid Organs
Here is the million-dollar question (literally): How do we keep the cells in the middle of a solid organ alive?
In a solid organ like the heart, liver, or kidney, cells are packed tightly together. Without a blood vessel right next to them, they die within minutes due to lack of oxygen. This is the diffusion limit—oxygen can only travel about 20 microns through tissue.
Why is this so hard?
Imagine trying to print a city where every house needs a direct water line. Now imagine that city is the size of a human heart, and the water lines are microscopic. That’s the challenge of vascularization.
Strategies to Solve the Vascularization Problem
1. Sacrificial Writing (SWIFT)
As mentioned earlier, the SWIFT technique from Harvard is a game-changer.
- Process: Print a dense block of living cells (Organ Building Blocks or OBBs). Then, use a sacrificial ink to print a network of channels. Finally, melt the sacrificial ink away, leaving behind a hollow network of channels.
- Result: You can create a 1cm thick tissue block with a functional vascular network.
2. 3D Bioprinting of Vascular Networks
Using multi-material bioprinters, scientists can print the structural cells (like cardiomyocytes) and the endothelial cells (which line blood vessels) simultaneously.
- Challenge: Getting the endothelial cells to self-asemble into functional, leak-proof vessels is difficult.
3. Decellularization and Recellularization
Instead of printing from scratch, take a donor organ, strip away all the cells (leaving the natural scaffold), and then repopulate it with the patient’s cells.
- Pros: Uses the organ’s natural, perfect vascular network.
- Cons: Hard to find donor organs, difficult to remove all cells without damaging the scaffold.
4. Angiogenesis Induction
Print the organ with growth factors that encourage the body’s own blood vessels to grow into the implant once it’s placed in the patient.
- Pros: Leverages the body’s natural healing.
- Cons: Slow, unpredictable, and may not be enough for large organs.
The Verdict: We are getting closer. The SLATE technology from Rice University has shown that we can print dynamic lung-like tissues with functional air sacs and blood vessels. But printing a whole, beating heart that can sustain a human life? That’s still a few years (or decades) away.
🔬 Current Breakthroughs: What We Can Print Today vs. Tomorrow
Let’s separate the hype from the reality. What can we actually do right now, and what is on the horizon?
What We Can Print Today (Clinical & Pre-Clinical)
- Skin Grafts: Used for burn victims. Companies like Poietis and Organovo are making strides here.
- Cartilage: For joint repair.
- Corneas: Early trials are showing promise for restoring vision.
- Liver Tissue (Mini-Livers): Not for transplant, but for drug testing. This is huge! Pharma companies are using these to test toxicity, saving millions on animal trials.
- Bone Scaffolds: Customized bone implants for craniofacial reconstruction.
What We Are Working On (The Next 5-10 Years)
- Heart Patches: Small patches of heart tissue to repair damaged areas after a heart attack.
- Kidney Tubules: Functional units of the kidney for drug testing and potentially dialysis support.
- Complex Vascular Networks: Better methods for creating the “plumbing” of solid organs.
The Future (10+ Years)
- Full Organ Transplants: A fully functional, 3D-printed heart, liver, or kidney ready for implantation.
- Personalized Medicine: Organs printed specifically for your DNA, eliminating rejection forever.
- On-Demand Printing: Hospitals with bioprinters on-site, printing organs in hours.
Enginer’s Insight: The transition from “organ-on-a-chip” to “organ-in-a-body” is the biggest leap. We need to solve the immune response and long-term durability issues first.
⚖️ Ethical Quagmires: The Moral Implications of Printing Human Organs
As we stand on the brink of this revolution, we must ask: Just because we can, should we?
The “Playing God” Debate
- Religious Perspectives:
Christianity: Some view it as stewardship (saving lives), others as encroaching on divine creation.
Islam: Focuses on preserving life, but questions the sanctity of creating life artificially.
Judaism: Balances Pikuach Nefesh (saving a life) with the sanctity of the human body. - Secular Ethics: Does creating artificial life blur the line between human and machine? What defines “human” if our organs are manufactured?
Equity and Access: The “Rich Man’s Organ”?
- Cost: If a bioprinted heart costs $50,0, will only the wealthy have access?
- Social Stratification: This could exacerbate existing health disparities, creating a world where the rich live longer, healthier lives while the poor wait for traditional donations.
Intellectual Property and Ownership
- Who owns the organ? The patient? The doctor? The company that designed the bioink?
- Patentability: Can you patent a human organ? The legal system is struggling to catch up.
Safety and Risk
- Unforeseen Consequences: What if the printed organ develops cancer? Or rejects the body in a new way?
- Testing: How do you test a custom-made organ before implanting it? You can’t test it on someone else!
A Thought to Ponder: If we can print organs, will we eventually be able to print enhancements? Imagine a heart that beats faster or a liver that detoxifies alcohol instantly. Where do we draw the line between therapy and enhancement?
💰 The Cost of Life: Economic Bariers and Future Accessibility
Let’s talk money. The current cost of bioprinting is astronomical.
Current Costs
- Bioprinters: $130,0 – $30,0+ for research-grade machines.
- Bioinks: $3.85 – $10+ per gram.
- Lab Setup: Sterile environments, bioreactors, and skilled personnel add hundreds of thousands more.
The Path to Affordability
- Open Source: Projects like the Open Biofabrication initiative are trying to create low-cost, DIY bioprinters.
- Mass Production: As demand grows, economies of scale should drive down costs.
- Recycled Materials: Using recycled polymers for scaffolds could cut costs significantly.
Prediction: In 20 years, the cost of a bioprinted organ could drop to a fraction of today’s price, making it accessible to the average person. But until then, it remains a luxury of the elite.
🛡️ Regulatory Roadblocks: FDA Approval and Safety Standards
The road to the clinic is paved with regulations.
FDA (USA)
- Current Status: No specific guidelines for 3D-printed organs yet.
- Approach: Regulated as Advanced Therapy Medicinal Products (ATMPs) or biological products.
- Challenge: The “custom-made” nature of bioprinted organs makes traditional clinical trials difficult. How do you run a double-blind study on a unique, patient-specific organ?
EMA (Europe)
- Classification: Bioprinted organs are classified as ATMPs.
- Stricter Rules: The EU has a more centralized approval process, which could slow down or speed up adoption depending on the outcome.
Global Landscape
- UK: Human Tissue Act prohibits commercial use of organs without consent.
- Japan: Has been more aggressive in approving regenerative medicine therapies, potentially leading the way in bioprinting.
The Bottom Line: We need flexible, adaptive regulations that ensure safety without stifling innovation. The current framework is too rigid for the rapid pace of bioprinting.
🌍 Global Landscape: Leading Labs and Companies in the Race
Who are the heavy hitters in this race?
Top Research Institutions
- Harvard Wyss Institute: Leaders in SWIFT and organ-on-a-chip technology.
- Rice University: Pioners in SLATE and vascular networks.
- Wake Forest University: Early pioneers in bladder and trachea printing.
- University of Minnesota: Developing 3D-printed heart valves and vascular grafts.
Leading Companies
- Organovo: Focused on liver tissue for drug testing.
- Cellink (now BICO): A major player in bioinks and bioprinters.
- Poietis: Specializing in laser-assisted bioprinting for skin and cartilage.
- Alevi (part of BICO): Offering a range of bioprinters and bioinks.
Fun Fact: Many of these companies are open-sourcing their designs to accelerate progress. Check out Thingiverse for some of the open-source bioprinter designs!
❓ Frequently Asked Questions About Bioprinting Human Organs
What are the current limitations of bioprinting human organs?
The primary limitation is vascularization. We can print the shape, but keeping the cells in the center alive is incredibly difficult. Other limitations include cell viability during printing, mechanical strength of bioinks, and the maturation time required for tissues to become functional.
How close are we to bioprinting a fully functional human heart?
We are likely 10-20 years away from a fully functional, transplantable human heart. We can print heart patches and valves now, but a whole heart with a complex vascular network is still a significant challenge.
What materials are used in bioprinting human organs?
We use a mix of natural polymers (collagen, alginate, gelatin), synthetic polymers (PEG, PLA, PCL), and living cells (stem cells, differentiated cells). The choice depends on the organ being printed and the desired properties.
Can bioprinted organs be rejected by the human immune system?
If printed with the patient’s own cells (autologous), the risk of rejection is minimal. However, if alogeneic cells are used, rejection is a major concern, requiring immunosupressant drugs.
How much does it cost to bioprint a human organ?
Currently, the cost is prohibitive, ranging from hundreds of thousands to millions of dollars per organ, including the printer, bioink, and lab time. However, costs are expected to drop significantly as the technology matures.
What ethical issues surround the bioprinting of human organs?
Key issues include equity of access (will only the rich get them?), ownership (who owns the organ?), safety (unforeseen risks), and religious concerns about “playing God.”
How long does it take to bioprint a human organ?
The actual printing process might take hours to days, but the maturation process in a bioreactor can take weeks to months before the organ is ready for implantation.
🏁 Conclusion
. This image represents ethics research understanding the human involvement in data labelling. It was created by Ariel Lu as part of the Visualising AI project launched by Google DeepMind. by 3D Printed")
We’ve journeyed from the humble beginnings of 3D printing plastic figurines to the cutting-edge frontier of bioprinting human organs. It’s a field that blends engineering, biology, and ethics in a way that feels almost like science fiction.
The Good News: We are making incredible progress. We can print skin, cartilage, and even complex vascular networks. The SWIFT and SLATE technologies have broken through the vascularization barrier, bringing us closer to the dream of printing solid organs.
The Bad News: We still have a long way to go. The vascularization of large, solid organs remains the biggest hurdle. Ethical, regulatory, and economic challenges lom large.
Our Verdict: Bioprinting is not a distant dream; it’s a reality in the making. While we may not be printing hearts for transplant tomorrow, the technology is advancing at a breathtaking pace. The next decade will likely see the first successful implantation of a 3D-printed organ, changing the course of medical history forever.
Final Thought: Remember that question we asked at the beginning? Why can’t we print a whole heart yet? The answer is vascularization. But thanks to innovations like SWIFT and SLATE, we are finally cracking the code. The future of medicine is being printed, one layer at a time.
🔗 Recommended Links
If you’re inspired to dive deeper into the world of 3D printing and bioprinting, here are some resources to check out:
Bioprinting Resources & Products
- 👉 Shop Bioinks & Bioprinters on: Amazon | BICO (Cellink) | Alevi
- 3D Models for Bioprinting Scaffolds: Thingiverse | Cults3D
Books & Educational Materials
- “3D Bioprinting: Fundamentals, Principles and Applications” on Amazon
- “The Future of Bioprinting” on Amazon
Internal Links from 3D Printed™
- Explore our guide to 3D Printable Objects for inspiration.
- Learn about 3D Design Software to create your own models.
- Read our 3D Printer Reviews to find the right machine for your needs.
- Discover how 3D Printing in Education is shaping the next generation.
- See how 3D Printing in Architecture is transforming construction.
📚 Reference Links
- 3D Bioprinting of Human Hollow Organs – PMC: https://pmc.ncbi.nlm.nih.gov/
- Wyss Institute – 3D Bioprinting: https://wyss.harvard.edu/technology/3d-bioprinting/
- UNOS – Organ Waiting List Statistics: https://unos.org/
- Rice University – SLATE Technology: https://bioengineering.rice.edu/
- FDA – 3D Printed Medical Devices: https://www.fda.gov/medical-devices/3d-printing-medical-devices/process-3d-printing-medical-devices
- BICO (Cellink) – Bioinks: https://www.bico.com/
- Organovo – Liver Tissue: https://organovo.com/
- Poietis – Laser Bioprinting: https://www.poietis.com/